
Last year I wrote a post called “The Starship and the Upstairs Flat” which concerns the longstanding (and until then, one-sided) relationship between the Sherlock Holmes and Star Trek canons. While working on that, I had cause to go have a look at the Sherlock DVDs, because in “The Blind Banker” we get a quick glimpse at John’s CV, and I wanted to examine it in detail.
(This was as much a harking back to old habits as mere curiosity. Nurses like to have the salient professional details about the doctors they know, and especially the ones they work with. Back in the day, when it was much harder to lay hands on pertinent details than just Googling for them, my colleagues and I were definitely not above quietly sending away for the State Board scores of doctors whose expertise we weren’t sure about.)
I hadn’t given much more thought to the subject until recently, when I had reason to look more closely at the Doctor’s CV. When I did, I began to realize that it says all kinds of interesting things about John Watson to a (former) health professional. Discussion follows…
My first pass at screencapping John’s info last year yielded a fair amount of useful data, but the middle of the page was hard to make out and I couldn’t then get much data out of it — which was annoying, as it held useful educational detail. But just this last week, when I took another run at the most difficult part of that middle page, I managed to make out most of the missing material (though still not absolutely everything, and I won’t bother uploading screencaps of the middle because it’s still way too fuzzy: the only way to read it was by watching it repeatedly in motion. BTW, you can click through these images for much bigger ones if you want).
So here’s what we have.
John’s description of himself:
“A conscientious reliable and hardworking medical professional, pays attention to details, crusader of clinical governance, with excellent intrapersonal and time management skills, seeking further training and experience in accident and emergency medicine while working toward a career in laparoscopic and bloodless surgery.”
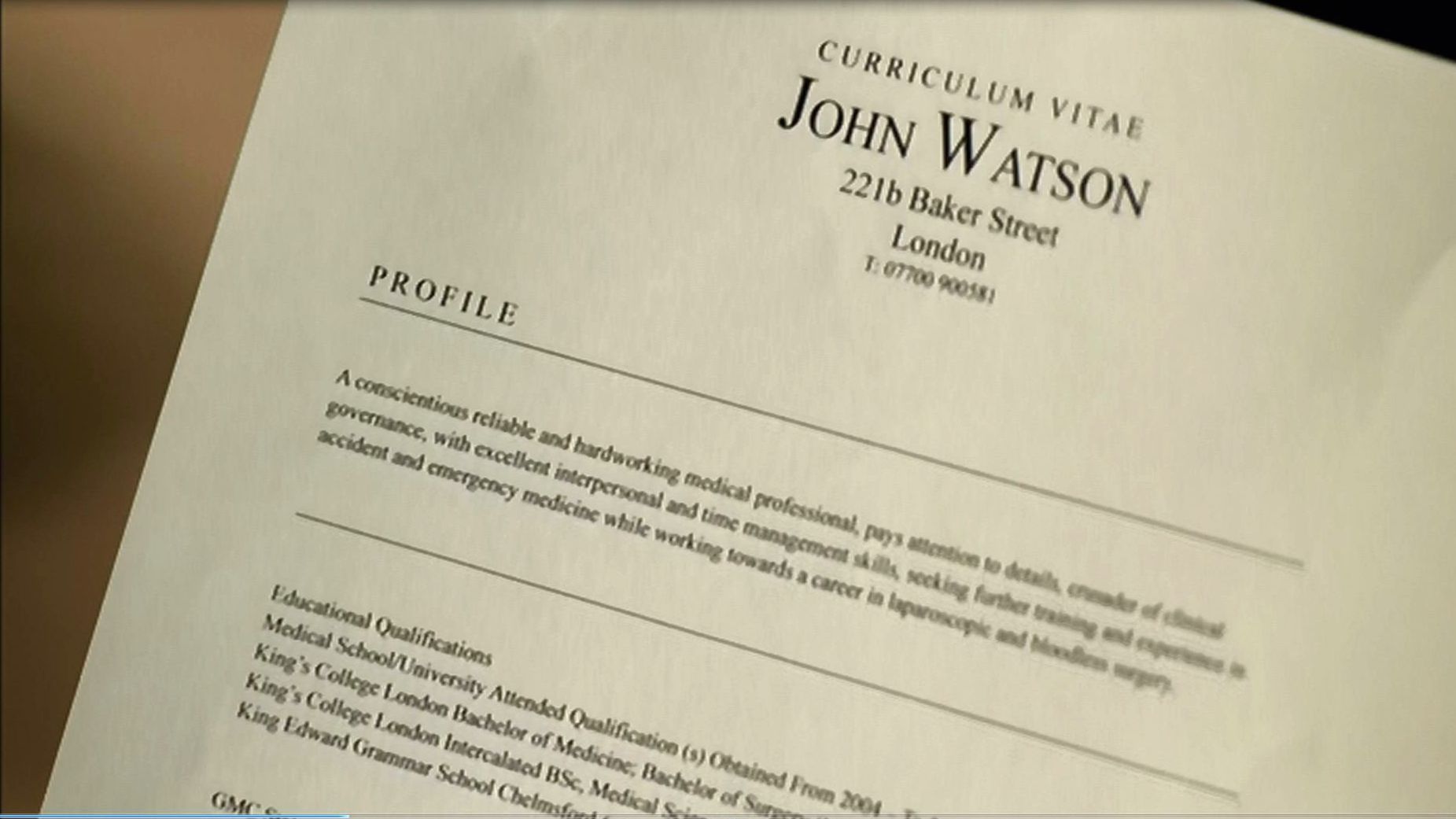
Now for the meat of it: details about John’s professional education, and his clinical training and experience. (Some of the educational details are visible above: others are in the part of the page that’s hardest to read because the camera in the insert is panning down.)
Educational Qualifications [these are in reverse order, most recent to least]
Medical School/University Attended | Qualification(s) Obtained From 2004 To 2006
King’s College London Bachelor of Medicine, Bachelor of Surgery (MBBS), 28/04/01 – 21/06/2004
King’s College London Intercalated BSc, Medical Sciences (Hons) 20/09/99[? hard to read] – 13/06/01
King Edward Grammar School, Chelmsford [couldn’t read the rest, but this is pre-uni and of less interest]
Registered with the General Medical Council [registration number unreadable]
Membership of Defence Union
Member, Medical Defence Union (EA566250)
Employment history:
University College* Hospital London PRHO General Surgery and Medicine (under Professor Barton[? hard to read] and Dr Collins) [no dates accompany this entry, but from the heading we might assume that he stayed until 2006]
Broomfield Hospital Chelmsford SHO Trauma and Orthopaedics (Under Mr. Taylor 04/02/05 – 02 / 06[?] / 05
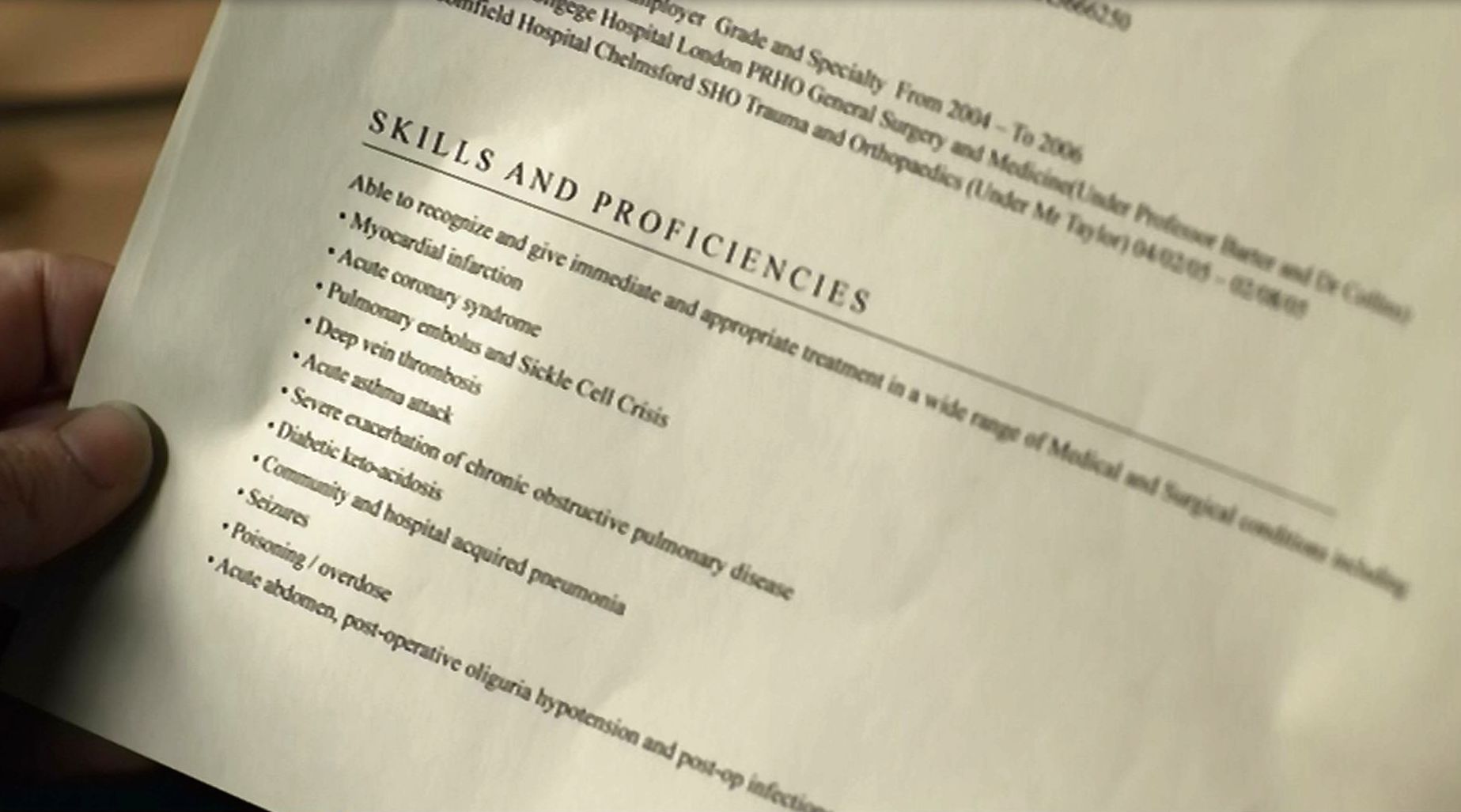
SKILLS AND PROFICIENCIES
Able to recognize and give immediate and appropriate treatment in a wide range of Medical and Surgical conditions including:
- Myocardial infarction
- Acute coronary syndrome
- Pulmonary embolus and Sickle Cell Crisis
- Deep vein thrombosis
- Acute asthma attack
- Severe exacerbation [sic: there should be another S in there] of chronic obstructive pulmonary disease
- Diabetic keto-acidosis
- Community and hospital acquired pneumonia
- Seizures
- Poisoning / overdose
- Acute abdomen, post-operative oliguria hypotension and post-op infection
…And that is all we have. “It says here you’re a soldier,” Sarah adds, but that data (dammit) is all on the next page.
So let’s deduce, and then speculate a little.
The dates themselves are the best place to start. John does the first part of his degree work, possibly with some premed (the Bachelor of Science in Medical Science, graduating with honors) between 1999 and 2001. He then starts his medical degree / surgeon’s degree in April 2001, before the award date for his BSc (this may simply be the way KCL structures its medical degree programs, rather than any sign of someone who’s insanely eager to get on with it). …A note here in passing: taking his medical degree from King’s College London, which is down in Southwark, does not necessarily conflict with canonical material that tells us John “trained at Bart’s”. Lots of medical (and nursing) colleges send their students to do clinical experience at other hospitals that are better suited to the unit of study in question. (When I was in nursing school, for example, my class was routinely bused all over Long Island to different hospitals depending on whether we were doing med/surg, OB/GYN, or whatever.)
So. John finishes his medical training in 2004. He then either takes time off, or jobhunts (or both) until February of 2005, when he goes to work at the hospital in Chelmsford; this is where he went to grammar school (and where I suppose we might safely assume he was raised). But he doesn’t stay there long. The month on the CV sheet is difficult to read, but by midsummer, or autumn at the very latest, he’s gone. Since no dates are given, there’s no way to tell when he started work at University College Hospital in London, but even if he started immediately on leaving Broomfield Hospital in Chelmsford and stayed right on through the end of ’06, he’s barely been at UCH in London a year before he’s moved on again.
We already know that John Watson is a smart young man, an honors graduate intent on constructing himself a clear pathway to a career that will engage him for life. John’s CV tells us that he’s “seeking further experience” in A&E and trauma medicine, indicating that this love affair has been going on from the start. But A&E work in London itself seems not to have been interesting enough for him in this regard … or maybe not exciting enough. What does a capable and ambitious young medical practitioner do in such a case?
He goes where large numbers of people are violently attacking each other, and the more frequently the better.
Leaving aside John’s Queen-and-country instincts toward patriotism and service (which Sherlock has noted, and John hasn’t really protested enough to suggest that Sherlock’s got it wrong), this is a very smart career move. If you want to become expert in trauma treatment and management, you take yourself somewhere that’s got lots of trauma. Granted, there are places in the UK that you could make a case would partially fill this bill. The Royal Victoria Hospital in Belfast, for example, is renowned worldwide for the expertise it’s been able to impart to its practitioners in the art of managing gunshot wounds and explosives injuries. But it seems this easy solution held no attraction for John. Maybe he was thinking: why go study trauma/A&E in a place that was (then) merely described as being like a war zone, when you could go study in a real one?
And there’s another issue here. Camp Bastion in Afghanistan is the world’s biggest, most cutting-edge field hospital, custom-built for its purpose — which is handling medical emergencies and aftercare for all the NATO and ISAF forces in the region. If you’re interested in studying trauma in depth, and under challenging circumstances, that sounds like a brilliant choice — the best way imaginable to acquire state of the art expertise. But they’re not going to let just any old doctor waltz in there. You have to be an army doctor.
So John enlists.
He enters the Fifth Northumberland Fusiliers (who are actually part of another regiment now) in… let’s assume early 2007… and does his military basic training with them. During this period he starts picking up what will plainly become a considerable expertise with small arms. Meanwhile his medical/surgical qualifications are being assessed by the Royal Army Medical Corps, to which he has applied to be seconded once he’s finished basic.
I don’t think the RAMC would have taken a long time over deciding they can really use him. John is well qualified as a surgeon, almost overqualified for a field surgeon, and definitely the kind of man they want — someone who plainly is not troubled by the prospect of being in harm’s way. Perhaps he’s even begun displaying something of a yen for being in the firing line… getting a bit hooked already, during his weapons training out on Salisbury Plain, on that potent drug, adrenaline. So the RAMC accepts him, commissions him some time in late 2007 or early 2008 as a captain (the normal starting rank for doctors in many world armed services) and ships him out to Afghanistan and the job of his dreams: that of a skilled trauma surgeon at Bastion.
We have no TV-canonical material to firmly support further speculation, but it seems very unlikely that someone with John’s skills and coolness under fire would be kept on base doing only theatre surgery. Doctors at Bastion also go out with medevac choppers to do pickup on ISAF and NATO wounded, and apparently are also sometimes seconded out for slightly longer periods to armed units. When not in theatre, therefore, John would have plenty of chances to continue honing his general weapons proficiency and his skill with the Sig, and to indulge his burgeoning love of danger and excitement, as he repeatedly gets shot at and gets better and better at shooting back. (Though the RAMC is not officially a fighting service — their regular-Army colleagues consider it their honor to defend RAMC personnel, who have other things to be thinking about on the battlefield — it’s understood that they do and will use their weapons in self-defense and/or the defense of their patients.)
And then, of course, finally it happens: John is shot, probably early in 2009 (possibly in an action coinciding with fallout from one of the traditional Afghanistan spring offensives). After recovering from whatever reconstructive surgery is required, and going through post-surgical physiotherapy, he’s invalided out in late spring or early summer of 2009 when it becomes clear that what appears to be PTSD has imparted an intermittent tremor to his dominant hand and left him with a psychosomatic limp — the former leaving him impaired for delicate surgery and the latter rendering him unfit for combat duty.
He returns to London and starts seeing his therapist in the autumn. And on 15 December, John posts for the first time in his blog: “Pointless.” Other equally desultory and unhappy postings follow, along with a couple that are meatier but still very sad, until the one that really interests us, on January 29, 2010: “A strange meeting”.
And then on the night of January 30th, the world’s only consulting detective — not realizing for just a few seconds who he’s talking about — describes John like this:
…That’s a crack shot we’re looking for, but not just a marksman: a fighter. His hands couldn’t have shaken at all, so clearly he’s acclimatized to violence. He didn’t fire until I was in immediate danger, though; so, a strong moral principle. You’re looking for a man probably with a history of military service and nerves of steel —
And then their eyes meet and realization sets in… and the rest, of course, is history.
The events that led up to this point would seem to have left their mark on the practitioner John intends to continue becoming. His CV clarifies the issue. Here we have a doctor who’s been marked by the exigencies of field surgery: a man who has apparently seen enough blood “to last a lifetime” and wants to alter his clinical path a bit. While he’s not abandoning his initial love of A&E and trauma surgery, he’s presently looking to exploit the recovered skill of his dominant hand — now, I think we can safely assume, tremor-free — in one of the most delicate scholia of surgery, laparoscopic work — so-called “keyhole surgery” or “bloodless surgery”. This is demanding work: a painstaking art that requires intimate knowledge of surgical tools that are increasingly subtle and complex. It is also the kindest of surgeries to the patient, causing far less pain and supporting much shorter recovery times. (And who knows, there’s a chance that a variant of such surgery was used on him, at Bastion, by colleagues with whom he’d been just hours earlier been practicing. It wouldn’t be the first time that a health professional has become better for his patients by suffering what they’ve suffered… by literally having a taste of his own medicine.)
We’ve already seen that in the first two seasons of his association with Sherlock, Dr. John Watson hasn’t had much leisure to go further down this road. It remains to be seen whether, in this regard anyway, his life after the Return will be much different.
I, for one, wouldn’t bet on it.
*Spelled “Collgege” in the original. Two possibilities here: (a) John’s non-speed-demon typing apparently cannot protect him from the occasional typo, and we can assume Sherlock didn’t see this document as he would inevitably have picked up on it. Or (b), the production staffer typing up the document made a mistake that no one else caught.